


 RELEASE DATE
RELEASE DATE
23.06.2022
 VALIDITY PERIOD
VALIDITY PERIOD01.01.2022 > 31.12.2022
Map
Projected Map
Other Projections




Key
results
Population
estimates
Recommendations
& next steps
Acute
Malnutrition
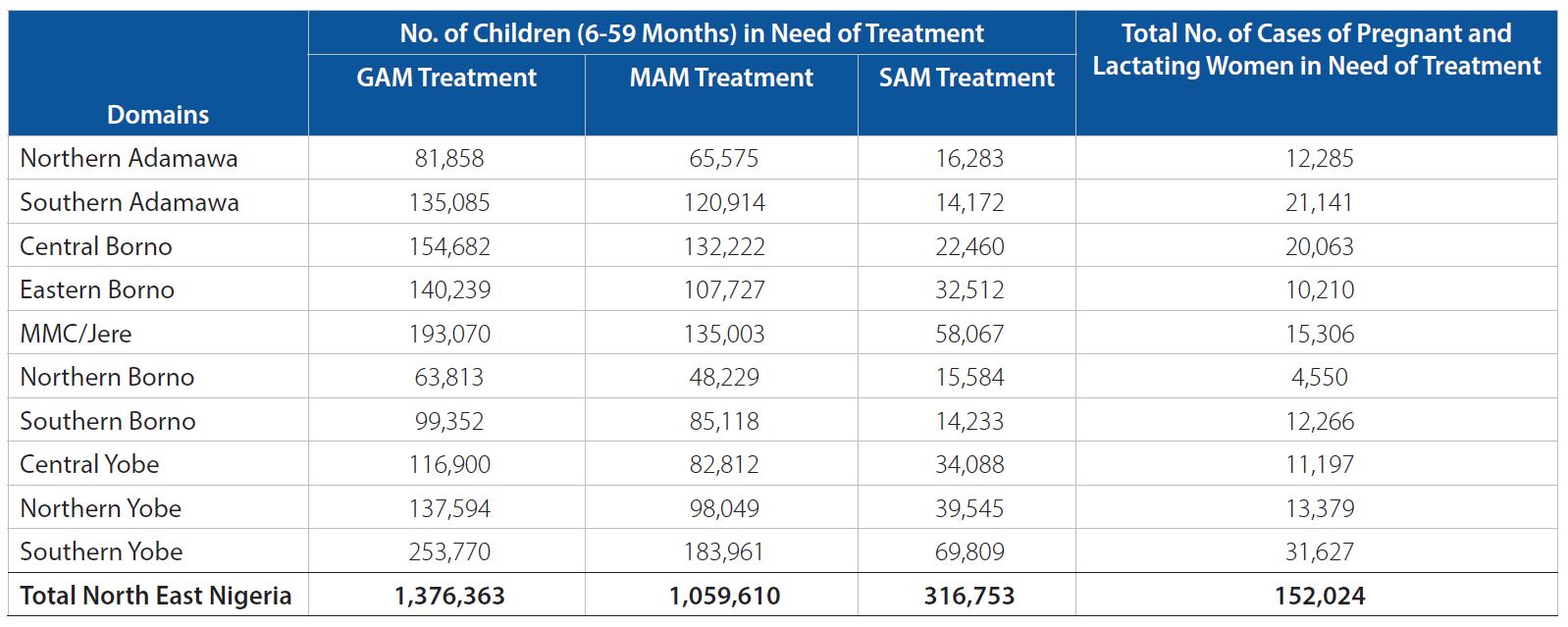
Over 1.3 million children under the age of five are expected to suffer from acute malnutrition in North East Nigeria between January and December 2022, based on the Global Acute Malnutrition (GAM) by Weight-for-Height Z-score (WHZ) prevalence estimates. This includes approximately 316,753 Severe Acute Malnutrition (SAM) cases and over one million Moderate Acute Malnutrition (MAM) cases. In addition, over 152,000 pregnant and lactating women will be acutely malnourished and need nutrition interventions.
Results of the IPC AMN analysis show that during the post-harvest season (a period of low acute malnutrition), only two (2) Local Government Areas (LGAs) are classified in a Serious situation (IPC AMN Phase 3), fifty-four (54) LGAs in an Alert situation (IPC AMN Phase 2), and five (5) LGAs in an Acceptable situation (IPC AMN Phase 1) between January and April 2022.
During the first projection (May – August 2022), which is the lean season and peak of acute malnutrition, the nutrition situation of 31 LGAs is expected to deteriorate, whereas the situation of 30 LGAs is expected to remain the same when compared to the current situation.
For the second projection period (September – December 2022), the harvest season (decreasing acute malnutrition), the nutrition situation is expected to improve in nine (9) LGAs, remaining the same in forty-two (42) LGAs and deteriorate in ten (10) LGAs when compared to the first projection period.
Country Related Information
Contacts
- 01.10.2025 > 30.09.2026
Nigeria (Northeast, Northwest and North Central): Acute Malnutrition Situation for October - December 2025 and Projections for January - April 2026 and May - September 2026 - 01.05.2024 > 30.04.2025
Nigeria (Northeast and Northwest): Acute Malnutrition Situation for May - September 2024 and Projections for October - December 2024 and January - April 2025 - 01.05.2023 > 30.04.2024
Nigeria (Northeast and Northwest): Acute Malnutrition Situation for May - September 2023 and Projections for October - December 2023 and January - April 2024 - 01.05.2022 > 30.04.2023
Nigeria (Northeast and Northwest): Acute Malnutrition Situation May - September 2022 and Projections for October - December 2022 and January - April 2023 - 01.09.2021 > 31.08.2022
Nigeria: Acute Malnutrition Situation September - December 2021 and Projections for January - April 2022 and May - August 2022 - 01.09.2020 > 31.08.2021
Nigeria: Acute Malnutrition Situation September - December 2020 and Projections for January - April 2021 and May - August 2021 - 01.09.2019 > 30.04.2020
Nigeria: Acute Malnutrition Situation in North East Nigeria September - December 2019 and Projection for January - April 2020
- 17.10.2025 > 24.10.2025
Nigeria: Acute Malnutrition Analysis - 17.08.2023 > 15.09.2023
Nigeria: Acute Malnutrition Analysis - 09.05.2022 > 16.05.2022
Nigeria: Acute Malnutrition Analysis - 08.11.2021 > 12.11.2021
NIGERIA: Acute Malnutrition Analysis

Join our mailing list