


 RELEASE DATE
RELEASE DATE
03.11.2019
 VALIDITY PERIOD
VALIDITY PERIOD01.05.2019 > 31.12.2019
Map
Projected Map
Other Projections



Key
results
Population
estimates
Recommendations
& next steps
Acute
Malnutrition
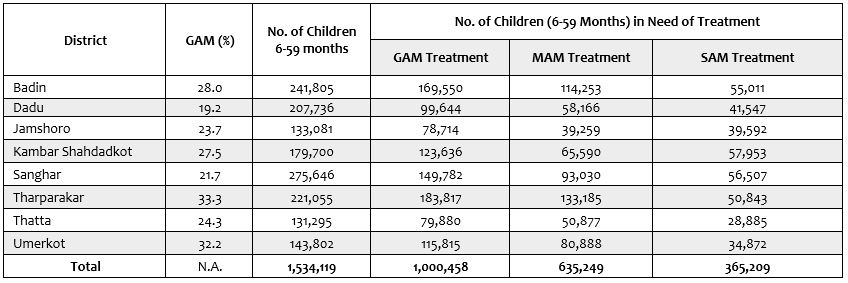
Acute malnutrition is a major public health problem in all the 8 drought affected districts in the Sindh province. Two districts in the province have Extremely Critical levels (IPC AMN Phase 5) of acute malnutrition – i.e. about every third child in these districts is suffering from acute malnutrition. Six other districts have Critical levels (IPC AMN Phase 4) of acute malnutrition. Although the 6 districts are classified in IPC AMN Phase 4, 2 of them have acute malnutrition levels very close to IPC AMN Phase 5.
Among the 8 drought affected districts notified by the Government of Sindh in 2018, the districts with Extremely Critical levels (IPC AMN Phase 5) of acute malnutrition are namely Tharparkar and Umerkot. The other 6 districts – Jamshoro, Kambar Shahdadkot, Badin, Dadu, Sanghar, and Thatta – are classified as being in IPC AMN Phase 4. Of these 6 districts, 2 of them, i.e. Kambar Shahdadkot and Badin, have acute malnutrition levels very close to IPC AMN Phase 5.
The major factors contributing to acute malnutrition include very poor quality and quantity of food, high food insecurity, poor sanitation coverage, and high incidence of low birthweight. Additionally, exclusive breastfeeding and access to safe drinking water are also of concern in several districts. Although not the direct focus of this analysis, anaemia among children of 6-59 months of age is at an alarming level.
Country Related Information
Contacts
- 01.10.2025 > 30.09.2026
Pakistan: Acute Malnutrition Situation October 2025 - March 2026 and Projection for April - September 2026 in Balochistan, Khyber Pakhtunkhwa and Sindh - 01.12.2025 > 30.09.2026
Pakistan: Acute Food Insecurity Situation for December 2025–March 2026 and Projection for April–September 2026 - 01.11.2024 > 31.07.2025
Pakistan: Acute Food Insecurity Situation for November 2024 - March 2025 and Projection for April - July 2025 - 01.03.2024 > 30.11.2024
Pakistan: Acute Food Insecurity Situation for March - June 2024 and Projection for July - November 2024 - 01.03.2023 > 31.01.2024
Pakistan: Acute Malnutrition Situation for March - September 2023 and Projection for October 2023 - January 2024 - 01.04.2023 > 31.01.2024
Pakistan: Acute Food Insecurity Situation for April - October 2023 and Projection for November 2023 - January 2024 - 01.07.2022 > 31.12.2022
Pakistan: Acute Food Insecurity Situation July - August 2022 and Projection for September - December 2022 - 01.10.2021 > 30.06.2022
Pakistan: Acute Food Insecurity Situation October 2021 - March/April 2022 and Projection for April/May - June 2022 - 01.04.2021 > 28.02.2022
Pakistan: Acute Malnutrition Situation in Sindh April - November 2021 and December 2021 - February 2022 - 01.03.2021 > 30.09.2021
Pakistan: Acute Food Insecurity Situation March - June 2021 and Projection for July - September 2021 in Balochistan and Sindh - 01.01.2020 > 31.08.2020
Pakistan: Acute Food Insecurity in Khyber Pakhtunkhwa January to May 2020 and Projection for June to August 2020 - 01.05.2019 > 30.11.2020
Pakistan: Acute Malnutrition in Balochistan May - August 2019 and Projection for September - November 2019 - 01.10.2018 > 30.11.2019
Pakistan: Acute Food Insecurity in Balochistan January - July 2019 and Projection for July - November 2019 and Sindh October 2018 - July 2019 and Projection for July - October 2019 - 01.04.2017 > 30.09.2017
Pakistan: Acute Malnutrition Situation April-June 2017 and Projection for July-September 2017 - 01.02.2017 > 04.08.2017
Pakistan: Acute Food Insecurity in Sindh Province February - August 2017 - 08.10.2014 > 18.12.2014
Pakistan: Acute Food Insecurity Situation October - December 2014 - 03.03.2013 > 31.03.2013
Pakistan: Acute Food Security Situation March 2013
- 31.01.2026 > 04.02.2026
Pakistan: Acute Food Insecurity and Acute Malnutrition Analyses - 11.12.2025 > 19.12.2025
Pakistan: Acute Food Insecurity & Acute Malnutrition Analysis - 14.11.2024 > 21.11.2024
Pakistan: Acute Food Insecurity Analysis - 04.03.2024 > 09.03.2024
Pakistan: Acute Food Insecurity Analysis

Join our mailing list